CPR Manikins, Training Tools, and Digital Simulation: A Life Support Coordinator Q&A

In this Q&A, we’re speaking with Tara Jett, MSN, RN, CMRSN. A life support coordinator and adjunct professor, Tara’s wide-ranging experience in curriculum development, staff mentorship, and healthcare technology has left her deeply familiar with the challenges involved in teaching and learning resuscitation.
Joining Tara in conversation is Hilary Gupte, RN, PGCE: a healthcare educator who has specialized in cardiac, critical care, and emergency settings.
Together, Tara and Hilary discuss:
- What makes resuscitation a hard process to learn and to teach from a physical, mental, and emotional standpoint
- The importance of the right CPR equipment, from manikins (informally known as CPR dummies) to automated external defibrillators
- How CPR manikins differ from digital simulation, and how the two complement each other
This Q&A has been adapted from a longer discussion. Responses have been edited, condensed, or rephrased for clarity and readability.
 Can you talk us through what makes resuscitation such a high-pressure skillset, especially for students or early-career nurses?
Can you talk us through what makes resuscitation such a high-pressure skillset, especially for students or early-career nurses?
TJ: Well, resuscitation is the first step in maintaining life in a situation where a patient is unconscious, responsive, not doing well, and so on. It’s about making sure we maintain circulation and oxygen delivery so their organs can keep functioning until we can reverse the cardiac arrest.
So, having the proper skills required to keep that circulation going can keep someone alive in those critical moments. It’s a high-stakes skill to learn.
What are some of the most common challenges you see when it comes to training for CPR and defibrillator use?
TJ: Maintaining the right CPR equipment is key. Because the fact is that you can’t practice on a person. If the CPR manikin is non-functional or unavailable, you can’t just say: ‘Right, lay down and we’ll push on your chest for two minutes!’. It’s just not feasible.
The other side of the coin, of course, is having the proper instructors on hand to make sure teaching and monitoring is done effectively. And it’s essential to make sure there’s consistency in the training, ensuring that all of the instructors are on the same page, held to the same standards, and understanding the essentials of what we’re teaching.
When instructors are willing to let learners off with a ‘you’re almost there’ due to time pressures, that’s not going to cut it: ‘almost there’ isn’t going to help someone who’s unresponsive and needs proper circulation and effective compressions.
HG: Instructor fatigue can also be a challenge. In my experience, assessing learners can be a really lengthy, repetitive process. You’re doing assessment after assessment in fifteen-minute intervals; by the end of the day, you barely know what you’re saying anymore!
MORE NURSING EDUCATION INSIGHTS | ‘Simulation Spotlight: ABCDE Assessments Q&A’
In your view, what separates textbook understanding from real-world readiness in resuscitation scenarios?
TJ: Frankly, it’s a highly emotional situation, and you have to be able to separate how you feel from the actual skill you need to exercise. And that’s made all the more challenging by the length of time codes can last: it can be a long time, and even when you’re switching out resuscitators every two minutes, it takes an emotional and physical toll. You can understand the skill through textbook learning, but you have to be able to feel the emotional element in training to prepare for real-life codes.
And in terms of continuing education, that’s why mock codes are something we’re pushing and trying to do more and more of throughout the year, instead of just waiting two years for everyone to recertify.
HG: That’s a really good point about the emotional education involved. So often we focus on the practical, tick-box elements of the skill and the percentage needed to pass. But doing this in real life, with an unresponsive patient on the end of your hands, is a very different ball game.
TJ: That’s a huge part of it. Because it’s great to know the steps, but if someone you know is turning blue, you react totally differently than to a CPR manikin—a piece of plastic, essentially—on the ground.
HG: And we do often teach resus and find that some people can end up performing CPR on relatives, not just patients. You might teach CPR to a dentist only to find that they never use it on a patient, but then they’re called on to resuscitate one of their parents. Lots of arrests do happen at home.
TJ: Absolutely. And, similarly, new parents will come in to take CPR training for the sake of their children. And while I can absolutely teach those steps, how do I teach you how to react when your child chokes and stops breathing?
HG: It’s about teaching through the emotion, not just the skill.
Are there any common misconceptions you encounter among learners when it comes to CPR protocols or AED usage?
TJ: They think it’s going to be easy. That’s the single biggest misconception: ‘oh, I can do this for two minutes.’ But two minutes is a very long time when you’re doing compressions, so that's a core element of the teaching process.
HG: And there isn’t much scope to vary your focus and concentration, is there? It takes a consistent pace and a consistent depth for the whole two minutes.
TJ: Absolutely. And you have to count out loud; that’s an essential part of the process. With each 30-second round of compressions, it gets harder and harder to count, which then throws everything else off. That’s why we train people to ensure that someone else is counting if needs be, ensuring everyone can hear.
 Where do you think traditional CPR training for nurses tends to fall short?
Where do you think traditional CPR training for nurses tends to fall short?
TJ: It all comes back to adding an emotional element into the training: learners are going to have to face (and push through) that side of the process.
In conjunction, though, there’s also a question of frequency. This isn’t a skill that you can refresh every two years and expect to maintain; it’s about muscle memory. In fact, there’s data suggesting that ER nurses—people who encounter codes more often—tend to have more successful results than those who work in other functions.
MORE ON NURSE TRAINING LIMITATIONS (AND HOW TO SURMOUNT THEM) | ‘Why Nursing Rotations Are Under Pressure (And How to Protect Student Readiness)’
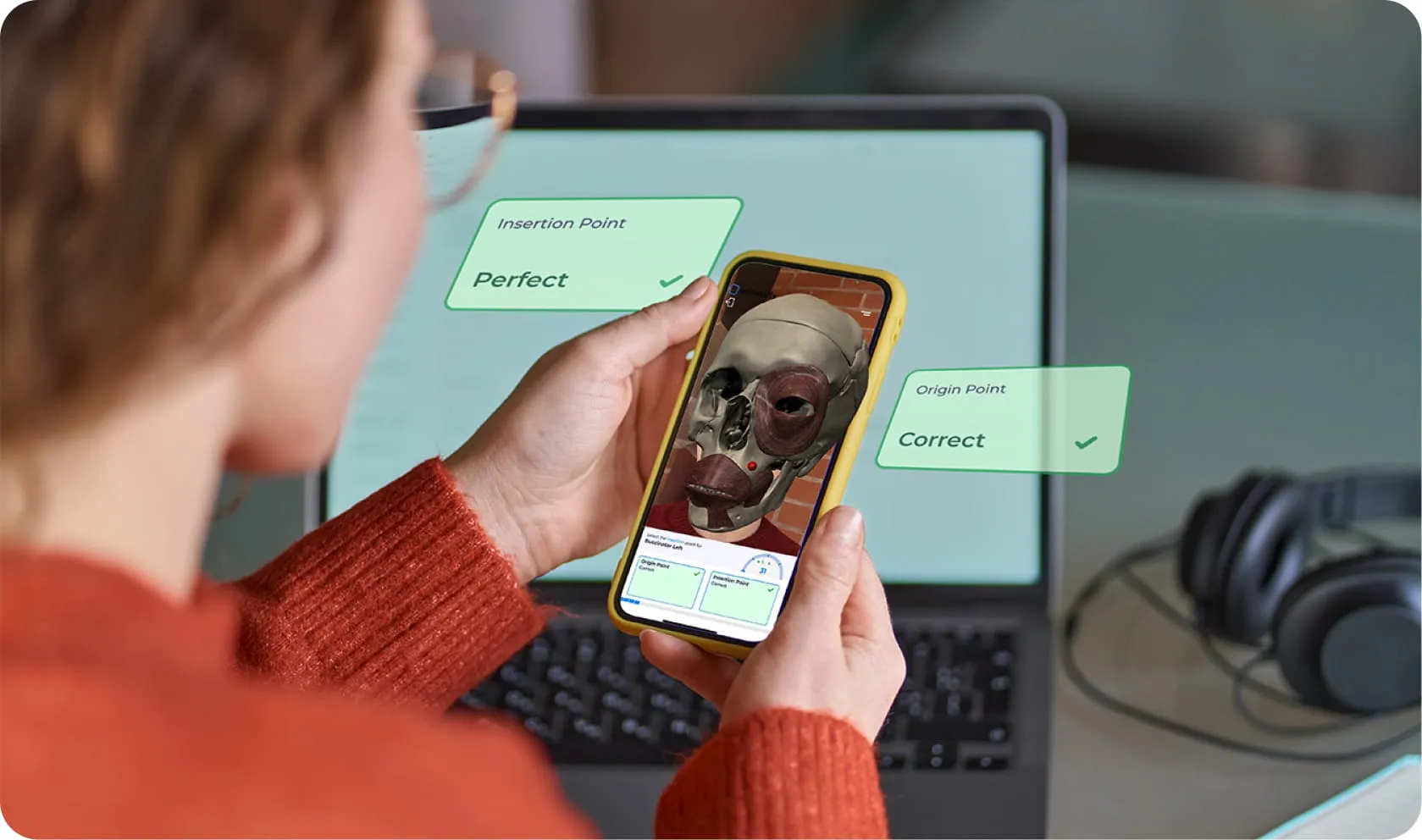
What value do you think digital or AR-based simulations offer when it comes to mastering resuscitation skills?
TJ: Digital simulation can’t fully replace traditional options, but there are absolutely areas where digital options perform better. We’ve talked about drawing out emotion, and the fact is that while the CPR manikins we use are great, they just don’t stir any kind of emotion.
But digital options are able to place resus into a scenario, rather than the physical skill.
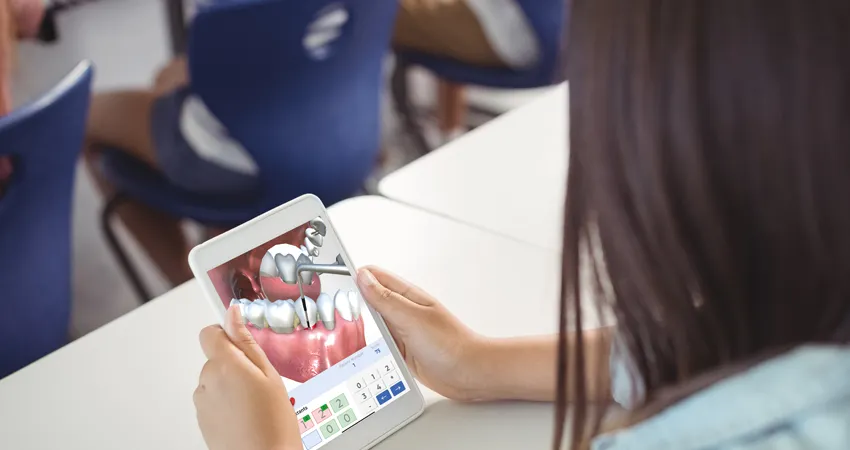
HG: I would say that with digital simulations, we can place the patient in a real setting and give some context to immerse the learner more than just practicing a skill on the classroom floor.
We can add alarms and interruptions and really try and make it feel a bit more real. Even if sticking to traditional resus updates, I would always try and provide a realistic scenario encompassing where the learner could find themselves in a resuscitation situation.
Both nursing students and professionals are adult learners. Does this inform your approach to teaching CPR?
TJ: Yes. As adult learners, it’s important to know and understand the ‘why’. There’s always a shortcut in nursing: somebody might point out a means of skipping five steps from a given process, and understanding why those steps are necessary can be the difference between keeping your sterile field uncontaminated or not.
And that applies to every practice we follow, really. Helping learners understand why chest compressions need to be a certain depth, especially ahead of time, is really necessary work.
HG: That’s another advantage of digital simulation, too: resources like a pre-resuscitation primer that allows you to visualize the heart compressing, see the recoil, and recognize the effects that has on the body is just something you don’t get from a CPR manikin, and it really illustrates that crucial question of ‘why’ we teach things a certain way.
What’s one thing you wish every nursing student knew about resuscitation before entering clinical placements?
TJ: The main thing I wish they knew is that they don’t know as much as they think! You might believe you know all the steps in the checklist, but putting it all together and making it function in a proper scenario is just essential.
And you have to remember that while code situations involve assigned roles, it’s not enough just to know yours. What do you do if someone’s at lunch? You have to be able to read the room and do what needs to be done. Ultimately, CPR is a horizontal effort, which really means frequent, continuous exposure to the theory and practice behind it.
Want to Add Digital Simulation to Your CPR Training Tools?
If you’d like to find out how expert-authored, curriculum-aligned nursing resources can reinforce and enhance the CPR manikins your institution uses with real-life urgency and internal visualization, you’re just a few clicks away.

Join our mailing list
Get the latest updates on immersive learning, industry trends, and resources delivered straight to your inbox.